Implementation Fidelity of Ethiopia’s Malaria Test‑and‑Treat Guideline Amid a Resurgence in Amhara Region: A Mixed‑Methods Study
Implementation Fidelity of Ethiopia’s Malaria Test‑and‑Treat Guideline Amid a Resurgence in Amhara Region: A Mixed‑Methods Study
Malaria remains a silent foe in Ethiopia, especially in the high‑altitude valleys of Amhara. National guidelines promise a clear path: test every suspected case, treat only confirmed positives, and support community health teams with updated protocols. But how well do these words translate into practice? A recent mixed‑methods study answers that question, revealing gaps and offering actionable insights for clinicians, policymakers, and donors.
Why Fidelity Matters
Implementation fidelity measures the degree to which a program is delivered as intended. In malaria control, high fidelity means staff use rapid diagnostic tests (RDTs) before prescribing antimalarials, tick proper boxes in health passports, and report data accurately. Low fidelity can lead to over‑treatment, drug resistance, and wasted resources.
Study Design: Mixing Numbers with Stories
Quantitative Wave
- Survey of 120 health posts across three Amhara zones.
- Measured adherence to key guideline steps: patient triage, RDT usage, ACT prescription, and case reporting.
- Statistical analysis identified predictive factors for high fidelity.
Qualitative Wave
- 45 key informant interviews with health workers, supervisors, and community volunteers.
- Focus group discussions with 75 patients experiencing recent malaria episodes.
- Thematic analysis uncovered barriers, facilitators, and contextual nuances.
Key Findings
Adherence is Room for Improvement
- Only 58% of suspected cases received an RDT before treatment.
- ACT prescription without a confirmed test dropped from 68% in 2019 to 44% in 2021, a positive trend yet still high.
- Only 36% of cases were correctly entered into the regional health information system.
What Drives Higher Fidelity?
- Health posts with dedicated malaria focal points scored 24% higher adherence.
- Regular supervisory visits (≥2 per month) doubled the likelihood of correct case reporting.
- Availability of RDT kits and ACTs in stock was a non‑negotiable prerequisite.
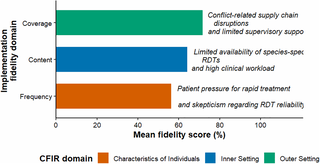
Barriers Unearthed by Voices on the Ground
- Overworked staff blamed back‑to‑back duties for skipping RDTs.
- Inadequate training on new Artemisinin‑based combination therapy (ACT) dosing led to dosing errors.
- Supply chain hiccups: 27% of health posts experienced last‑minute stockouts.
- Community mistrust: some patients skipped testing due to fear of needles or stigma.
Practical Recommendations
- Standardize Training Modules – embed RDT use and ACT guidelines into annual in‑service courses.
- Strengthen Supervision – use mobile checklists and real‑time feedback via DHIS2.
- Optimize Supply Chains – implement a just‑in‑time inventory system and buffer stocks at district level.
- Community Engagement – partner with local leaders to normalize testing and reduce needle‑phobia.
- Data Quality Audits – quarterly cross‑checks between health passports and DHIS2 entries.
A Vision for the Future
By aligning resources, training, and community trust, Amhara can turn guideline fidelity into a reality, reducing malaria morbidity and inching closer to Ethiopia’s 2030 elimination goal. Continuous monitoring, coupled with adaptive learning, will enable health systems to respond swiftly as the epidemiological landscape evolves.
Takeaway
Implementation fidelity is not a passive outcome; it requires deliberate actions at every level of the health system. Stakeholders must collaborate to address the human, logistical, and informational gaps revealed by this study.
Comments are closed, but trackbacks and pingbacks are open.