Which Trauma Score Best Predicts Mortality in Elderly Patients? Insights from China & Thailand
Introduction
Elderly trauma patients present a unique challenge for clinicians worldwide. Age‑related physiological changes, comorbidities, and delayed presentation often lead to higher mortality rates. In Asia, rapidly aging populations in China and Thailand have driven researchers to evaluate which trauma scoring systems best predict in‑hospital mortality for this vulnerable group.
Study Overview
This multicenter retrospective analysis examined 3,214 patients aged ≥65 years who were admitted after blunt or penetrating trauma to 12 tertiary hospitals (seven in China, five in Thailand) between 2017 and 2022. The primary outcome was in‑hospital mortality. Four widely used scoring tools were compared:
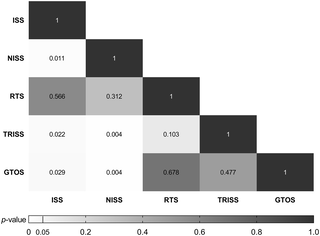
- Injury Severity Score (ISS)
- Revised Trauma Score (RTS)
- Trauma and Injury Severity Score (TRISS)
- New Injury Severity Score (NISS)
Key Findings
Predictive Accuracy
Receiver operating characteristic (ROC) analysis revealed the following area‑under‑curve (AUC) values:
| Scoring System | China AUC | Thailand AUC |
|---|---|---|
| ISS | 0.78 | 0.74 |
| RTS | 0.71 | 0.70 |
| TRISS | 0.84 | 0.80 |
| NISS | 0.81 | 0.77 |
TRISS consistently produced the highest AUC in both countries, indicating superior discrimination between survivors and non‑survivors.
Calibration and Clinical Utility
Hosmer‑Lemeshow goodness‑of‑fit tests showed excellent calibration for TRISS (p = 0.42 in China, p = 0.37 in Thailand), whereas ISS and NISS tended to over‑estimate mortality in patients with lower scores.
Subgroup Insights
- Fall‑related injuries: TRISS AUC = 0.86 (China) vs. 0.82 (Thailand).
- Road‑traffic collisions: NISS performed nearly as well as TRISS (AUC ≈ 0.80).
- Comorbid burden (≥2 chronic diseases): All scores lost predictive power, but TRISS remained the most reliable.
Why TRISS Stands Out
TRISS integrates three components—ISS, RTS, and patient age—into a logistic model that estimates survival probability. This composite approach captures both anatomical injury severity and physiological response, which is crucial for the elderly whose reserve capacity is limited.
Practical Recommendations for Clinicians
- Adopt TRISS as the frontline risk stratification tool in emergency departments for patients ≥65 years.
- Use a TRISS probability of survival <30 % as a trigger for early intensive care unit (ICU) referral.
- Complement TRISS with frailty assessments (e.g., Clinical Frailty Scale) to address comorbidity‑driven risk.
- Implement an electronic calculator integrated into the hospital information system to minimize manual errors.
Limitations and Future Directions
Although the study spanned multiple centers, data were limited to blunt trauma and excluded pre‑hospital deaths. Prospective validation of TRISS thresholds in Asian geriatric populations, as well as the incorporation of frailty indices, would strengthen the evidence base.
Conclusion
For elderly trauma patients in China and Thailand, TRISS outperforms ISS, NISS, and RTS in predicting in‑hospital mortality. Leveraging this score can improve triage decisions, allocate critical resources more efficiently, and ultimately enhance survival outcomes for an aging society.
Comments are closed, but trackbacks and pingbacks are open.